

We would all be more likely to administer a poison if the antidote were immediately available.
After watching this video it’s obvious there’s numerous factors at play. One may conclude this has nothing to do with Sugammadex – rocuronium was never administered – this is the point for discussion.

(40seconds post propofol administration – unable to insert LMA)
To state Sugammadex could have saved Elaine Bromiley may cause some consternation. However, a proportion of anaesthetists will nod in agreement. They may be fortunate to work in an environment where Sugammadex is readily available – among their emergency drugs, next to suxamethonium, some of these anaesthetists draw up rocuronium.
Why?
Perhaps primarily to overcome functional airway obstruction (the situation that occurred early in the Elaine Bromiley case). These anaesthetists don’t hesitate to administer rocuronium early. In the video some see themselves administering rocuronium as little as 40 seconds after propofol administration, facilitating insertion of the laryngeal mask.
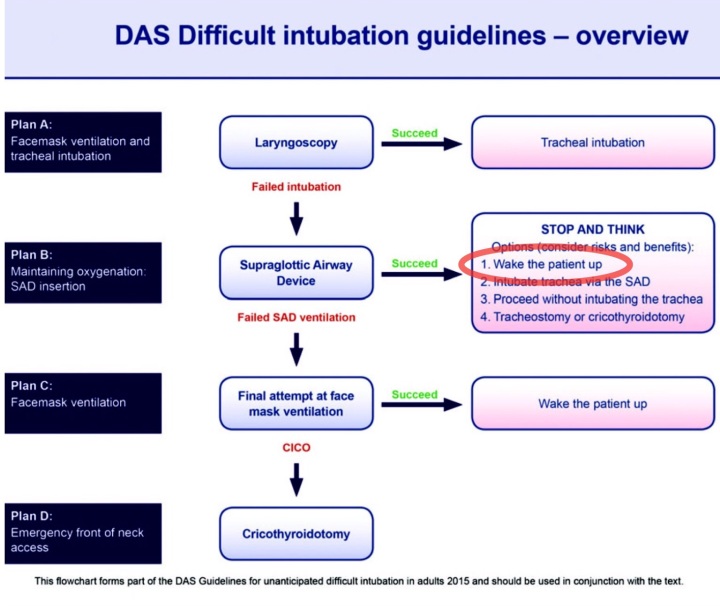
Others however elect to deepen anaesthesia, and may attempt to insert the LMA while the patient is resisting. They may traumatise the airway, potentially converting functional airway obstruction into mechanical airway obstruction. Their actions may create a ‘can’t intubate can’t oxygenate‘ situation.
Why not just give suxamethonium? Well some do – it was given in this case 4 minutes and 15 seconds after propofol administration – at this stage there is profound hypoxia and bradycardia. Why wait this long? There are many reasons including belief the situation will improve with deepened anaesthesia, concerns about myalgia in an elective case, arrhythmias, denial things aren’t as bad as they seem….
In this situation if we give rocuronium, with Sugammadex immediately available, we have nothing to lose.
Sugammadex is an enabler. We are more likely to paralyse our patients when Sugammadex is immediately available.
So why do some institutions still not have immediate in theatre access to sufficient Sugammadex?
2 reasons:
1. Cost
Our hospitals are obliged to protect the finite healthcare dollar. MSD / Merck need to supply Sugammadex at a price that is not restrictive.
Signing this petition may encourage them to do this.
2. Late Adopters
Late adopters proclaim we’ve given anaesthetics for years, without Sugammadex, and without related problems. Hospital administrators, hearing from them that immediate access to Sugammadex is unnecessary, are quick to listen.
However if administrators listen instead to anaesthetists understanding the human factors approach to patient care we may avoid another Elaine Bromiley case.
The box of Sugammadex doesn’t even need to be opened, just immediately available, enabling anaesthetists to confidently paralyse their patients early – this level of safety hasn’t really cost anything.
Prior to Sugammadex anaesthetists were unable to rapidly reverse deep levels of paralysis. Immediately after an induction dose of rocuronium, using its competitor neostigmine one would have to wait approximately 40minutes. Sugammadex if given in sufficient dose (10 vials in 125kg patient) will reverse paralysis in approximately 2 minutes. This is a rare requirement but will happen.
Immediate access to sufficient Sugammadex gives anaesthetists the confidence to paralyse patients providing optimal airway conditions.
Trials have shown that when Sugammadex is locked up in a central location it takes almost 7 minutes to obtain in an emergency (that’s if the keys can be located and the cupboard has been restocked) – by then it’s too late.
Please, for patient safety, do not lock up Sugammadex and have a sufficient dose (1 box of ten x 200mg vials) available on each theatre drug trolley.
Patientsafe has no financial interest with Merck / MSD / Sugammadex or any of the other products we discuss on our website.
For more information please read on….
‘No longer should Sugammadex be kept hidden away centrally in some locked cupboard, but available immediately to hand in the anaesthetic/operating room.’
See: Editorial of 2015 Difficult Airway Society Guidelines.
Sugammadex is overpriced – sign the petition for a price reduction.
Immediate (in theatre drug trolley) Sugammadex will benefit rapid reversal where a patient’s deteriorating airway can just be ventilated:
‘We found that costly time was lost because sugammadex was not directly available in the operating theatre. This decision was made at a managerial level because sugammadex is an expensive drug.’ (See Anaesthesia Sept 2010)
Understandably hospital administrators have warmed to those anaesthetists proclaiming immediate access to Sugammadex is unnecessary – it takes the pressure off them and their budget – this is very short sighted as there are numerous hidden cost benefits to Sugammadex (see here). This in turn leads to stress on front line staff members who understand immediate access is in the interest of optimal patient management.
There are several reports of successful Sugammadex use in airway rescue: (see here) However it’s vital we educate its use is unreliable in airway emergency. It is unlikely appropriate in a CICO situation. For those pre-emptively considering its use when managing a difficult airway perhaps understand that an alternative approach will be more suitable.
It’s intuitive, that in rare cases of airway rescue if rapid reversal may benefit, a sufficient dose of Sugammadex needs to be immediately available in the theatre drug trolley.
A box of 10 vials of 200mg Sugammadex ensures a 16mg/kg dose for patients weighing up to 125kg.
The cost of Sugammadex restricts availability. From our understanding the cost of a 200mg vial in Australia varies from A$45 to 195 depending on contract agreements.
There are institutions who do not purchase it, and others who only make it available from a centrally located locked cupboard.
We present a tiered approach to Sugammadex restriction which limits use but ensures immediate availability in sufficient dose:
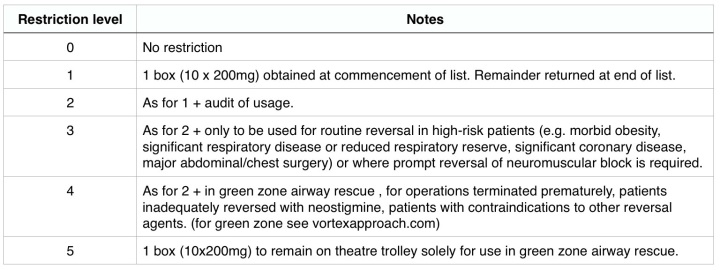
We hope that healthcare institutions adopt this approach enabling optimal patient safety while allowing for current cost constraints.
How you can help:
1. Ensure your institution has immediate access (in theatre drug trolley) to sugammadex so it may be rapidly drawn up to reverse a large induction dose of rocuronium (1.2mg/kg).
2. Offer to perform an audit of Sugammadex usage.
3. Sign the petition requesting Merck reduce the price.
4. Forward any interesting anecdotal cases where the presence or absence of Sugammadex may have had a significant impact (avoid any identifiers).
5. For those colleagues still undecided about the benefits of unrestricted access to Sugammadex provide a link to the following article:
Sugammadex – What Price Are We Willing To Pay?
While Merck did not develop Sugammadex, through a series of acquisitions they now control the price.
Sugammadex is overpriced.
This is detrimental to patient care and places unnecessary stress on hospital staff. We should encourage Merck to reduce the price so we may all benefit from unrestricted access. This is after all their company mantra:
We ask that Merck do the right thing – the healthcare community won’t forget their decisions – we can only hope that Merck remember ‘medicine is for the people‘.
Sign the petition requesting Merck reduce the price.
We sent this letter to the CEO of Merck on 21st May 2016 – we await his reply.
Please note that patientsafe has no financial interest with Merck (MSD) or Sugammadex.

I don’t use Rocuronium. Never have after its first year of its introduction. But how often does the need to be in this scenario to rapidly reverse muscle paralysis??
But it it was available at a realistic price would it convince other Anaesthetists to switch to rocuronium? Is that a better marketing ploy for MSD to improve use to Rocuronium and more profits? This would fit their motto then!
LikeLike
If you are concerned, why not use succinylcholine, a cheap effective paralytic that only lasts a few minutes? That seems more practical than using a long-acting paralytic and an expensive reversal agent that works in a few minutes?
LikeLike
Hi Robert, If you watch the video you will notice that they did use suxamethonium – but after 4 minutes. I must admit this is likely what I would have done, trying to avoid something which might cause myalgia and other issues until I was absolutely sure I needed it in a completely elective patient. With sufficient sugammadex in the background I see the junior trainees extremely willing to paralyse patients much earlier with rocuronium than they would with suxamethonium – they have pretty much nothing to lose in this situation. If you look at the vortex approach to airway management yo will notice they mention that each step has not failed unless the patient is paralysed. We need to give our anaesthetists the confidence to paralyse early in the event of airway difficulty – they get this confidence by having the box of sugammadex in the room.
LikeLike
I’m not sure when bridion was available I know it’s not been too long. So unsure it was available when ELAINE had her anaesthetic. It’s all here say. In that situation it’s always difficult. Easy for us to make comments….. at least Elaine’s husband can rest assured we are more alert to this problem. As an educator we use Elaine’s story as teaching aid. I was still questioned a few weeks back when I called for help when two senior consultants were struggling with an airway. I felt I had to apologise…..crazy I know. I did too and the drs were grateful I had called for help……..
LikeLike
Thanks Maggie for the comment. We need to improve our ability to work in teams and be more confident to speak up. We need to flatten the hierarchy somewhat to allow this to happen. Unfortunately cases like Elaine’s still play out throughout the world. The psnetwork.org is working towards providing the best front line environments for staff to provide optimal care. Having a box of Sugammadex immediately available allows for this. Thank you again. Rob
LikeLike